DERMATOMYOSITIS
This is an E log book to discuss our patients de identified health data shared after guardians informed consent.
Here we discuss our individual patient problems through series of inputs from available global online community of experts with an aim to solve this patients clinical problems with collective current best evidence based inputs.
This E-book also reflects my patients centered online learning portfolio and your valuable comments in comment box are most welcome.
Details of patient when admitted 2 months back in a health centre in the below link:
https://rhea9895.blogspot.com/2022/01/29-years-old-female-with-co-joint-pains.html
Reference of this blog: Reference:https://nikitha0510.blogspot.com/2022/03/dermatomyositis.html?m=1)
I have been given this case to solve in an attempt to understand the topic of "patient clinical analysis" to develop my competency and to comprehend clinical data including history, clinical finding investigations and come up with a diagnosis and treatment plan.
Chief complaints:
Fever since 4 days
Cough since 4 days
B/L joint pains associated with pedal oedema since 4 days
Dyspnoea since 3 days

HISTORY OF PRESENTING ILLNESS
Patient was apparently asymptomatic 12 months ago.
Then she developed symmetrical b/l joint pains in the knees which was insidious in on set, gradually progressive, no aggravating factors and relieved on medication
she developed itching over neck and upper chest area and due to over it hing at the location it turned black.


(Reference:https://nikitha0510.blogspot.com/2022/03/dermatomyositis.html?m=1)
Alopecia since 12 months associated with pain,
Also had malar rash which was initially erythematousbut later became hyperpigmented.

vaginal discharge since 10 months. It was initially curdy white which later changed to watery discharge
Difficulty in walking.distal muscle weakness
She also had difficulty in breathing at rest since 3 days.which was gradually progressing
. She also complained of pins and needles sensation in the palms and thighs.
.
PAST HISTORY
No H/O DM, HTN, asthma, epilepsy, CAD
Personal history:
Diet ;mixed
Sleep adequate
Bowel,bladder habits regular.
Addictions none.
Menstrual history:
Menarche: 11 year
Cycle lasts: 26-28 days
3 days of menstruation
Regular cycles
She also had vaginal discharge.
No pains or clots:
MARITAL HISTORY
She is married but doesn't have any kids, she has adopted a girl from her sister in law
She has primary infertility.
GENERAL EXAMINATION
The patient was conscious, coherent, cooperative, well oriented to time, place, person. She was moderately built and moderately nourished
Pallor: Present
No icterus, cyanosis, clubbing, lymphadenopathy
Pedal edema: present
VITALS:
Temperature: afebrile.
BP: 150/100 mm Hg
PR: 114 bpm
RR: 30 cpm
SYSTEMIC EXAMINATION
CVS - S1, S2 hear
RS: BAE +
P/A: soft, non tender
CNS: NA
Investigation:

They performed a ANTI NUCLEAR ANTIBODY immunofluorescence which showed
Homogeneous pattern. Intensity 4+ the assosiated antigens involved are: dsDNA, Histones.
They also performed an HRCT which showe
: few patchy areas of ground glass opacities in peri bronchovascular distribution- s/o pneumonitis
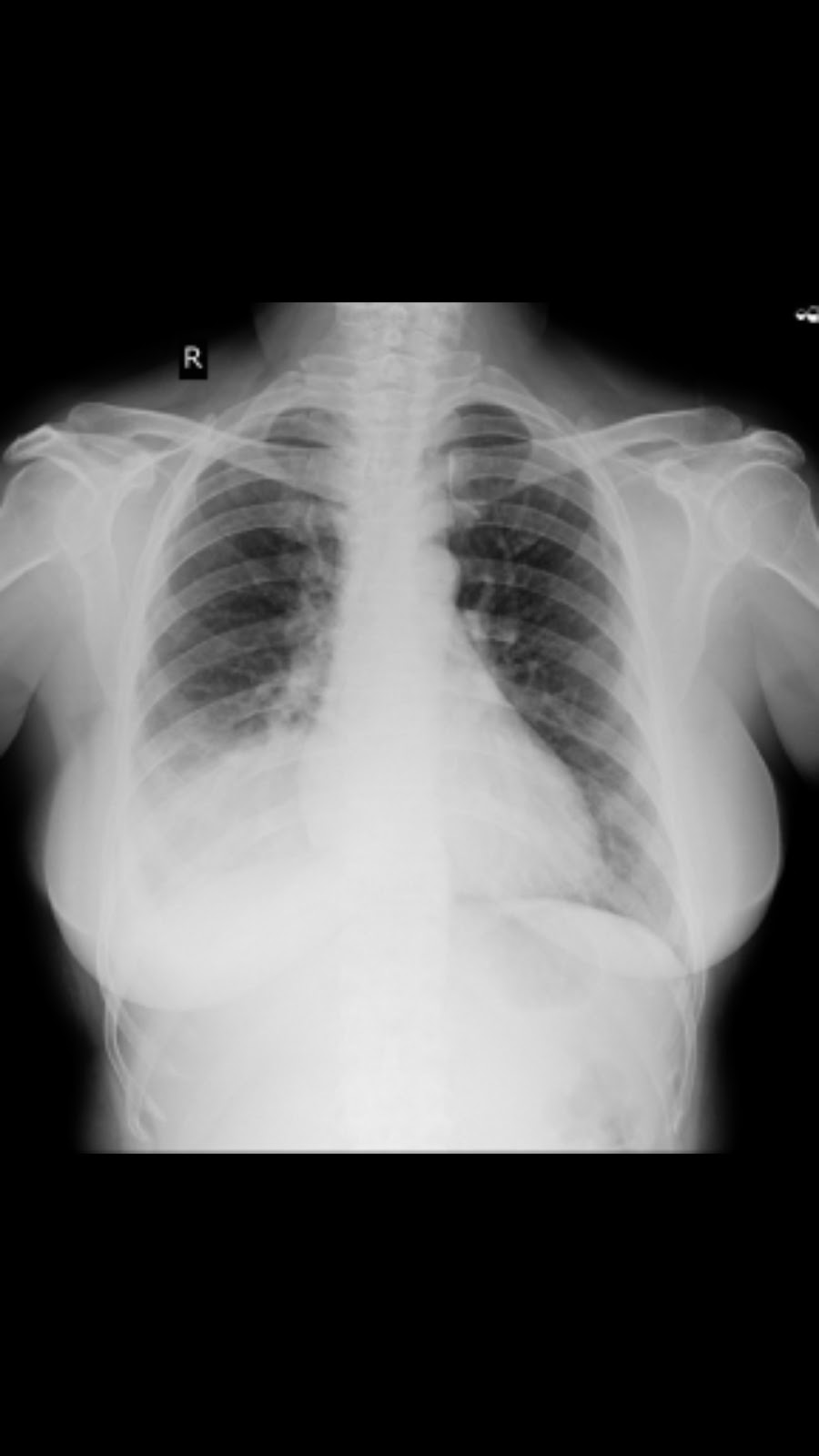
Chest xray.:
PROVISIONAL DIAGNOSIS
DERMATOMYOSITIS with candidiasis.
TREATMENT:
1.T.SEPTRAN DS TID
2.TAB.FLUCONAZOLE 150 MG OD
3.OINT.CANDID.
4.TAB.WYSOLONT 50 MG OD
5.TAB.FOLIC ACID 5 MG ONCE A WEEK.
Images after 2 months of treatment:


Present images.:



Key points:
Heliotropic rash : diffuse erythematous hyperpigmented motted patch.
Shawl sign: rash extended upto neck and back.
Holsier sign: macule on the groin.
Gotrin papules: pigmentation on knuckles.


Comments
Post a Comment